

Lowdown on Continuous Lactate Monitors
Lowdown on Continuous Lactate Monitors
Everything you need to know about the intricacies of the next big biowearable


Image from Goodwin et al
For those in the wearables and health tech space, there was quite some buzz around continuous lactate monitors following Abbott’s announcement at CES in 2022 that they will be releasing one. At the time I took notice, and I eagerly await their release, but it feels like they’re is getting more and more hype in the general population. Once I have been asked my thoughts more than once, I figure writing about it is a good idea - so here we are.
NOTE: I have tried to keep this as brief as possible but it’s as long as is necessary to explain some concepts and to be relevant to all audiences - thus requiring some more explaining. Those with some background or knowledge in the space will be able to skip portions like ‘what is lactate’ and maybe ‘lactate metabolism’. For a more comprehensive article on lactate itself and testing in athletes, check out Sean Seale’s work here.
What is Lactate?
Long thought to be a metabolic waste product (and cause the burn we associate with intense exercise), in a classic case of “correlation isn’t causation”, this couldn’t be further from the truth for lactate. It is one of the most fascinating molecules in the body serving as a metabolical intermediary, a fuel and playing a role in cell signalling. Emerging evidence is also showing it plays a significant role in the brain may also have a role in psychiatric care (for those interested, check the references below).
Put simply, lactate is the end product of breaking down carbohydrates and links glycolytic (aka anaerobic) metabolism with oxidative metabolism (aka aerobic).
What is a Continuous Lactate Monitor?
A continuous lactate monitor (CLM) is a biowearable that will continuously measure lactate levels in the body. This will replace lactate monitoring which is traditionally done in a more discrete manner, in both the health and performance spaces.
Traditionally lactate is sampled via blood, in a healthcare/hospital setting this is often part of blood testing. In a performance (and at times health) setting this is often via pricking a finger or earlobe and sampling this capillary blood with a lactate meter.
Quick Glossary of Terms:
Interstitial fluid (aka IF or ISF) - fluid that surrounds cells (see below)
Capillary - small blood vessel, these supply the skin (eg what bleeds when you get a paper cut)
Kinematics (as used in this article) - movement and dynamics of a substance
Glucose - simple sugar we use in the body (a simple form of carbohydrate)
How Will They Work?
I don’t know EXACTLY how they will work, but they will sample the interstitial fluid, which is a fluid that surrounds cells and serves as an interface between cells and the blood (see below graphic). They will likely have a reagent that reacts with lactate (probably lactate oxidase for the record), and then convert this reaction into a signal, which is then equated to a lactate value (see second image below).
, which is a type of extracellular fluid (ECF). The fluid in the blood vessel is also an example of extracellular fluid. The fluid in the cytoplasm of each body cell is intracellular fluid, or ICF.")
Image Source
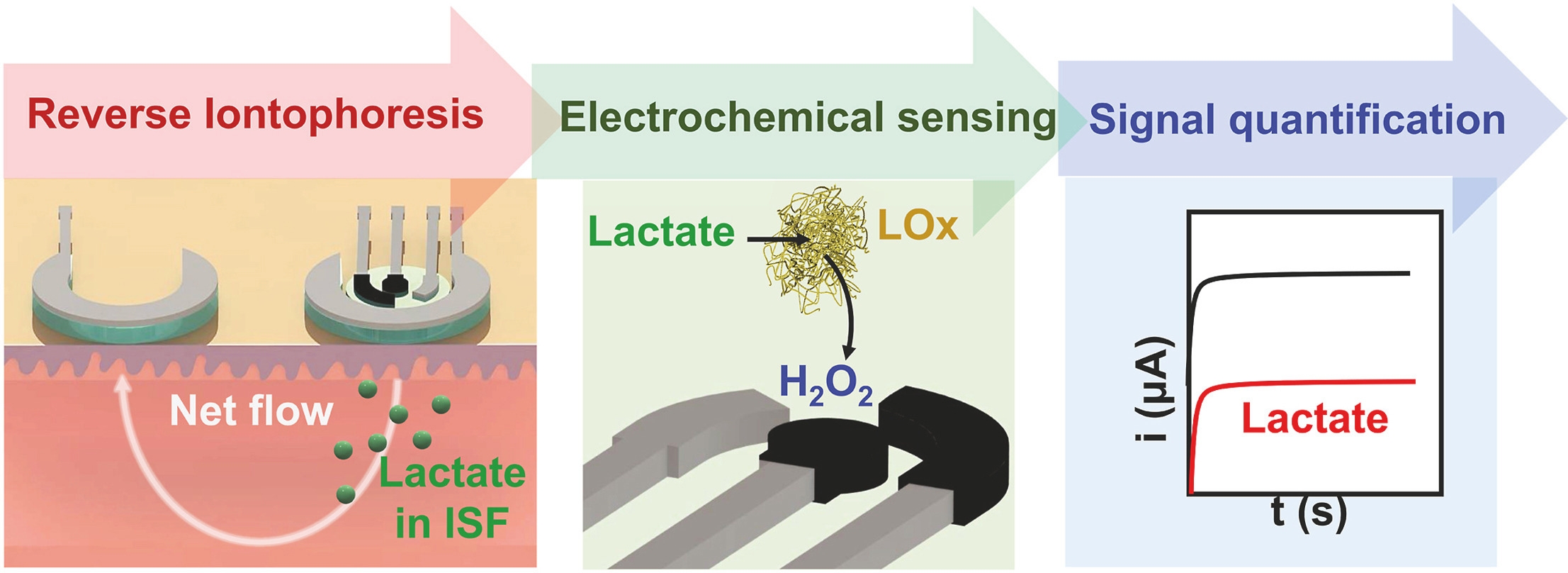
From De la Paz et al
In this was they’ll be very similar to continuous glucose monitors, which are currently widely available to both people with, and increasingly without, diabetes. In a similar fashion they will probably have an applicator involving a needle introducing the sampling filament into the interstitial fluid and last for something like 1-2 weeks before needing replacing.
What are the use cases for Continuous Lactate Monitors?
There’s a little bit of ‘built it and they will come’ here but I do think there are some very natural use cases. The majority of people who are reading this, or even those who have heard about these CLMs, likely predominantly thought about their use in a sporting context but there health use cases likewise.
Performance
Current use of lactate in a performance context is almost exclusively for endurance endeavours and amounts on roughly two broad uses:
1) Designation of intensity - understanding physiological thresholds with relevance to energy systems and substrate (carbs or fat) utilisation.
2) Intensity control - ensuring current intensity is appropriate given number 1.
This is a gross oversimplification but is sufficient for our purposes.
CLM use will mirror this in the initial period of time on the market. From there, people will start to track it serially to better understand readiness, adaptation and as another datapoint to add to a suite of datapoints being tracked for health of the athlete. For the record, I think the tracking of adaptation (or maladaptation - think overtraining type scenarios) is where the real value will be for most.
See a broader ‘take’ on where CLM data will head below.
Health
In a situation I have always found fascinating, many metrics (for example metabolites and vital signs) are very similar in both exercise (more extreme specifically) and disease. This, of course, includes lactate which is often an indicator of severe illness in the healthcare setting. Thus, it is often monitored somewhat serially - enter CLMs.
Interestingly, I heard reports from medical friends still working clinically, that the aforementioned continuous glucose monitors were used to track glucose in patients during the COVID-19 pandemic to limit need to sampling blood for glucose values. It doesn’t take much imagination to envisage both of these becoming standard of care at some point.
Beyond the healthcare setting, in a health space, there is increasing interest in so called “zone 2 training”. Without opening a can of worms, for many people a CLM could help in both discerning the rough intensity of exercise required for achieving this and ensuring this intensity is adhered to (for those who understand lactate metabolism intimately please don’t send me hate mail - I am trying to keep this simple).
The Challenges Continuous Lactate Monitors will Face
Having seen first hand the challenges continuous glucose monitors have faced, I think there will be some parallels that CLMs and their adoption will face.
Questions of Accuracy
Understanding of lactate has historically been through the lens of blood, which whilst similar to measures of interstitial fluid, is not always the same (for more see below section on lactate metabolism). As a result CLMs will face questions of accuracy when values differ from lactate meters used by athletes for example.
This is, in my mind, well intentioned (of course we need some sort of anchor on whether what we are seeing is accurate) but misguided. This is because as a result of a different sampling location (yes interstitial fluid communicates directly with blood but it’s not the same) and as a result different kinematics.
Understanding Kinematics
As mentioned any one lactate value may be questioned from an accuracy standpoint when comparing lactate meters and CLMs but the physiology of the two sampling sites is different. This means that what we understand of lactate metabolism needs to be updated when referencing the the different fluid compartments (blood and interstitial fluid). On that note, blood itself varies by site of sample.
I recently had the privilege of spending some time with Olav Aleksander Bu (one of the world’s preeminent endurance coaches and someone synonymous with lactate in many people’s minds) where we discussed CLMs. We were in violent agreement on the challenges CLMs will face (though he was a little less positive about them than I am). His view is that even the two traditional sites of lactate sampling in athletes; the earlobe and the finger, show a significant difference in values in certain situations. For example, he mentioned in cross country skiers he suggests using the earlobe given the significant role the arms play (thus the values at the finger are impacted). Now consider this when comparing a different sampling fluids.
Lenses of Understanding
The aforementioned parallels here with continuous glucose monitors need clarifying for their utility. Historically continuous glucose monitors were used in people with diabetes, and our understanding of blood glucose was through the lens of blood and diabetes. NOT through interstitial fluid and people without diabetes. This means our understanding is through a vastly different lens, and with the uptake of continuous glucose monitors in people without diabetes, this understanding has been challenged and change quickly. The parallel here being that ‘normal’ or ‘normative’ with be very different for CLMs to lactate meters and our time to understand the time taken to understand this will not be insignificant. There will be some who do not bother to take the time to understand them and will write them off I am sure and some who decide they’d prefer to stay with more traditional methods of testing.
We will also have visibility on a range of time we previously did not have. For example, we have rarely had much lactate data overnight during sleep. It is foreseeable that this could be a trove of information, perhaps with respect to recovery and adaptation, perhaps improving accuracy of sleep wearables etc. It may too show us some things we didn’t account for, for example a high lactate value at a time that is surprising. This will take time to understand - see my advice for use of these below.
Lactate Metabolism
I will do what I can to keep this simple but accurate.
Lactate is produced to some degree at all times. When intensities of exercise increase so does lactate (because you progressively burn more carbohydrates as intensity goes up), with two more distinct “thresholds” (which have more names than the phone book, but most commonly lactate thresholds 1 & 2 or aerobic & anaerobic thresholds).
In the main image for this article at the top you can see that Ra (rate of appearance) increases relatively linearly with intensity of exercise. Likewise, Rd (rate of disappearance) goes up relatively linearly (though their rates are different. La (or lactate) is the net of these two processes; production and disappearance. This is important because the curve we see (and what so much of endurance physiology is based off of) is somewhat a function of WHERE we sample.
Lactate is produced primarily in working muscle (where the carbohydrates are burned), it can then be shuttled elsewhere to be reconverted into glucose and used. This is why despite ongoing lactate production we don’t see huge increases in measured lactate initially but again - this would differ based on site of sample (working muscle would be different to a distant site.
When exercise intensity exceeds our ability to shuttle this lactate elsewhere we start to see an increase in lactate. As mentioned before there are two distinct thresholds where we see changes in rate of change of lactate accumulation (eg upticks). Beyond the latter of the two thresholds we see significant accumulation of lactate (one of the many aforementioned names of this point is OBLA or “onset of blood lactate accumulation”).
Different profiles of individuals from a metabolism standpoint will have different curves of lactate and training can change them (see this for more). Better ability to burn fat (sometimes termed metabolic flexibility) and a more developed aerobic system (enter zone 2 training) will mean lower resting baseline lactate levels and lower lactate for longer (as you body can better use it and shuttle it away). This does go somewhat hand in hand with being a more “slow twitch” or endurance type of athlete. This may seem a little ‘in the weeds’ (and yes I enjoy nerding out on this stuff) but it has relevance to use of CLMs in health. Metabolically unhealthy people may see somewhat high lactate levels at rest, and may see rises in these levels at low work intensities - both of which can be addressed and improved through training.
When it comes specifically to disease I won’t go into the intricacies of exactly what’s driving lactate production (that’s a textbook chapter not a newsletter), but suffice to say, lactate levels can be very high and stay elevated for a large portion of disease pathology.
Noise in the Data
Lactate data can be very noisy and getting accurate samples is more difficult than most appreciate. This is particularly pertinent in current lactate sampling in athletes and is less relevant in the hospital setting. This is because lactate is a concentration, which means contamination is a huge concern (in fact there are companies looking to use sweat lactate as a non-invasive measure). Even if the sample is well taken, the noise in lactate data is significant with day to day variance reported of ~30% at times. Now, it should be noted, that some of this variance (maybe a lot of it) could be signal rather than noise, that is - the source of this difference is meaningful (for example hydration status). Just because the noise is meaningful (and thus not truly noise) doesn’t mean users will find it helpful, in fact, in my experience the level of detail and nuance in this will cause many to discard CLMs rather than spend time to understand the nuance.
My Take on the Future of CLMs
There will be a huge initial surge in media and interest in these devices, followed by a backlash against them (my hunch is questions of accuracy and arguments they’re not needed by anyone other than elites).
They are technically already banned by the UCI in racing - but this will definitely be a story.
As with most of these sorts of devices and data streams, there will be a number of features (and scores etc) built on top of the data after a period of time.
It will take while for companies and individuals to start understanding what ‘normal’ is with continuous data and this may initially drive some users to feel as though there is something wrong with them (see below for my advice on this).
There will be many researchers jumping at the opportunity to use these in research, my hunch being overtraining and altitude will be the areas of most interest initially. On this note, this research will be released at least 12 months after they are on the market - that’s the timeline for science (and an optimistic one).
I am interested to see what we can learn from lactate with respect to sleep specifically and the use of CLMs in addition to continuous glucose monitors to better understand the metabolic picture more holistically.
At some point we are likely going to see the Apple Watches of the world look to develop (or buy a company that has developed) non-invasive lactate sensing. This will probably be once CLMs have seen some good market traction.
Advice to New Users of Continuous Lactate Monitors
Start from the basis of observation (not intervention) ie collect and observe data, don’t change anything initially. This will help you understand your normal in context of your life and lactate data.
Assume you are normal, not abnormal ie what you’re seeing is more likely physiological not pathophysiological. So don’t jump at shadows. The obvious exceptions being if you are sick (or could be) or if for some reason you are indeed not “normal” and that’s why you’re using a CLM.
Corroborate your data. Use other sources of data that should work in concerto with lactate for example RPE (rating of perceived exertion) and heart rate. This will help better understand the data in general and factors such as reliability and accuracy. It may also help understand kinematics.
Once you understand YOUR normal; start to characterise your extremes to get a more rounded picture of the spectrum of your physiology. You will need to test multiple times given how noisy lactate data can be.
*Disclaimer: I previously worked for a company that sells continuous glucose monitors which also may have had some access to continuous lactate monitors but I have not had any inside information on them nor have I had access to them and this has not informed my thoughts in this article. These are my thoughts and opinions alone.
References
Goodwin ML, Harris JE, Hernández A, Gladden LB. Blood lactate measurements and analysis during exercise: a guide for clinicians. J Diabetes Sci Technol. 2007 Jul;1(4):558-69. doi: 10.1177/193229680700100414. PMID: 19885119; PMCID: PMC2769631.
Brooks GA, Arevalo JA, Osmond AD, Leija RG, Curl CC, Tovar AP. Lactate in contemporary biology: a phoenix risen. J Physiol. 2022 Mar;600(5):1229-1251. doi: 10.1113/JP280955. Epub 2021 Feb 25. PMID: 33566386; PMCID: PMC9188361.
Brooks GA, Osmond AD, Arevalo JA, Duong JJ, Curl CC, Moreno-Santillan DD, Leija RG. Lactate as a myokine and exerkine: drivers and signals of physiology and metabolism. J Appl Physiol (1985). 2023 Mar 1;134(3):529-548. doi: 10.1152/japplphysiol.00497.2022. Epub 2023 Jan 12. PMID: 36633863; PMCID: PMC9970662.
Wu A, Lee D, Xiong WC. Lactate Metabolism, Signaling, and Function in Brain Development, Synaptic Plasticity, Angiogenesis, and Neurodegenerative Diseases. Int J Mol Sci. 2023 Aug 29;24(17):13398. doi: 10.3390/ijms241713398. PMID: 37686202; PMCID: PMC10487923.
Rabinowitz JD, Enerbäck S. Lactate: the ugly duckling of energy metabolism. Nat Metab. 2020 Jul;2(7):566-571. doi: 10.1038/s42255-020-0243-4. Epub 2020 Jul 20. PMID: 32694798; PMCID: PMC7983055.
Lee S, Choi Y, Jeong E, Park J, Kim J, Tanaka M, Choi J. Physiological significance of elevated levels of lactate by exercise training in the brain and body. J Biosci Bioeng. 2023 Mar;135(3):167-175. doi: 10.1016/j.jbiosc.2022.12.001. Epub 2023 Jan 19. PMID: 36681523.
Caddye, E.; Pineau, J.; Reyniers, J.; Ronen, I.; Colasanti, A. Lactate: A Theranostic Biomarker for Metabolic Psychiatry? Antioxidants 2023, 12, 1656. https://doi.org/10.3390/antiox12091656
Li, X., Yang, Y., Zhang, B. et al. Lactate metabolism in human health and disease. Sig Transduct Target Ther 7, 305 (2022). https://doi.org/10.1038/s41392-022-01151-3
Brooks GA. Lactate as a fulcrum of metabolism. Redox Biol. 2020 Aug;35:101454. doi: 10.1016/j.redox.2020.101454. Epub 2020 Feb 9. PMID: 32113910; PMCID: PMC7284908.
De la Paz E, Saha T, Del Caño R, Seker S, Kshirsagar N, Wang J. Non-invasive monitoring of interstitial fluid lactate through an epidermal iontophoretic device. Talanta. 2023 Mar 1;254:124122. doi: 10.1016/j.talanta.2022.124122. Epub 2022 Nov 25. PMID: 36459870.
Yogev, Assaf & Arnold, Jem & Nelson, Hannah & Clarke, David & Guenette, Jordan & Sporer, Benjamin & Koehle, Michael. (2023). Comparing the reliability of muscle oxygen saturation with common performance and physiological markers across cycling exercise intensity. Frontiers in Sports and Active Living. 5. 10.3389/fspor.2023.1143393.
Hi David another extremely insightful article, particularly in how it demystifies lactate's role in the body and illuminates the potential of continuous lactate monitors (CLMs) in transforming both athletic performance and healthcare monitoring.
I can't help but wonder about the role of Generative AI (GenAI) and Artificial General Intelligence (AGI) in this context. How much of an impact could these technologies have on the development and integration of CLMs and similar health technologies? Could GenAI and AGI further enhance the accuracy, functionality, and user experience of these devices, or perhaps even revolutionize the way we interpret and act on the health data they provide? It's an exciting time and I look forward to seeing how these fields will collaborate to push the boundaries of what's possible.