


Tattoos in Health and Performance
A look into tattoos in the realms of health and performance


Tattoos have well and truly transitioned from the realms of the rebellious and criminal into what seems to be the norm (research I read in writing this piece suggested prevalence rates of 20-30% - this would clearly slant younger but it’s still surprisingly low to me). This change has been somewhat generational but regardless, it certainly seems that those without tattoos are the exception in 2025. This situation; one where the prevalence of a behaviour changes, creates an interesting opportunity from a natural experiment standpoint. Another example that comes to mind, and in a somewhat similar timeframe, is that of the cervical cancer vaccine.
In these types of situations, where there was a base rate of a behaviour and a subsequent change in said behaviour, we can observe changes in prevalence of known, or unknown outcomes as an indication of risk factors and mechanisms. In one of these cases, the vaccination case, the behaviour is actually an ‘intervention’ due to some mechanistic understanding of a specific pathology (cervical cancer) and thus tracking is both necessary but also easier (because the outcome of interest - cervical cancer rates - is a known one). In the case of tattoos, outcomes are less easy to be sure of but some physiological understanding can give us some insights in places to monitor.
What Happens When Someone Gets a Tattoo
I will spare readers the absolute basics here; ink, tattoo gun which delivers thousands of little droplets of ink, pain, mild bleeding etc. Most would also understand that the pain is very location dependant - they’re generally more painful in areas that are more densely innervated (hands, soles of the feet etc).
Some key things, which are much less talked about, happen with tattooing. It’s worth noting tattoos are an injury, or at least the body would see it that way, and as such there is an immune system response. This response, as is always the case, has an acute phase (seconds to days) and a more chronic response (months and years) which is not always the case for all injuries. The acute response settles and the more chronic response is what allows dispersion and persistence of tattoo ink (see details below). Fundamentally this revolves around macrophages (they’re an immune cell - we aren’t going into it, immunology is amazing but it’s complicated) some of which hang around filled with tattoo ink some of which go to the lymph nodes.

The key here is understanding that the body never recognises the tattoo ink as ‘self’ - a key delineation in the immune system and response. In short; ‘self’ is safe and the body mounts no response, where as ‘non-self’ is unsafe and warrants an immune response. Without getting into the ‘how’ of this, it is a malfunction in this (self vs not self) which causes autoimmune disorders. It probably goes without saying that the inability to eliminate this ‘non-self’ stimulus is probably less than ideal. What this means is something we are discovering more and more.
Performance
Far from a purely negative, tattoos have long traditions in warrior cultures for good reason. They certainly have a role to play in intimidation and psychology - which shouldn’t be underplayed. It’s also hard to go past the phrase: “look good, feel good” (sometimes extended to: “look good feel good, feel good play good, play good pay good).
The downside of tattoos in a performance realm is sweating. There is evidence suggesting that tattoos impair the skin’s normal sweating response - which can be a huge issue in performance. Remembering humans are uniquely evolved to dissipate heat (anthropologists suggest the lack of fur and ability to sweat to dissipate heat were key factors that allowed us to capture and kill animals - via exhaustion hunting), with evaporation of sweat being one of four potential means for us to do this (the others being convection aka wind, conduction aka heat transfer via direct contact and radiation aka heat transfer without direct contact).
The research in the space has come from one group predominantly and some of their results are visualised below (from 2 different studies). We won’t get much into the details but it is worth noting that the impact of tattoos is very heterogenous (and to be honest, sweating is too). This may be an artefact of how we measure sweating which is, as you can imagine, not that straight forward.

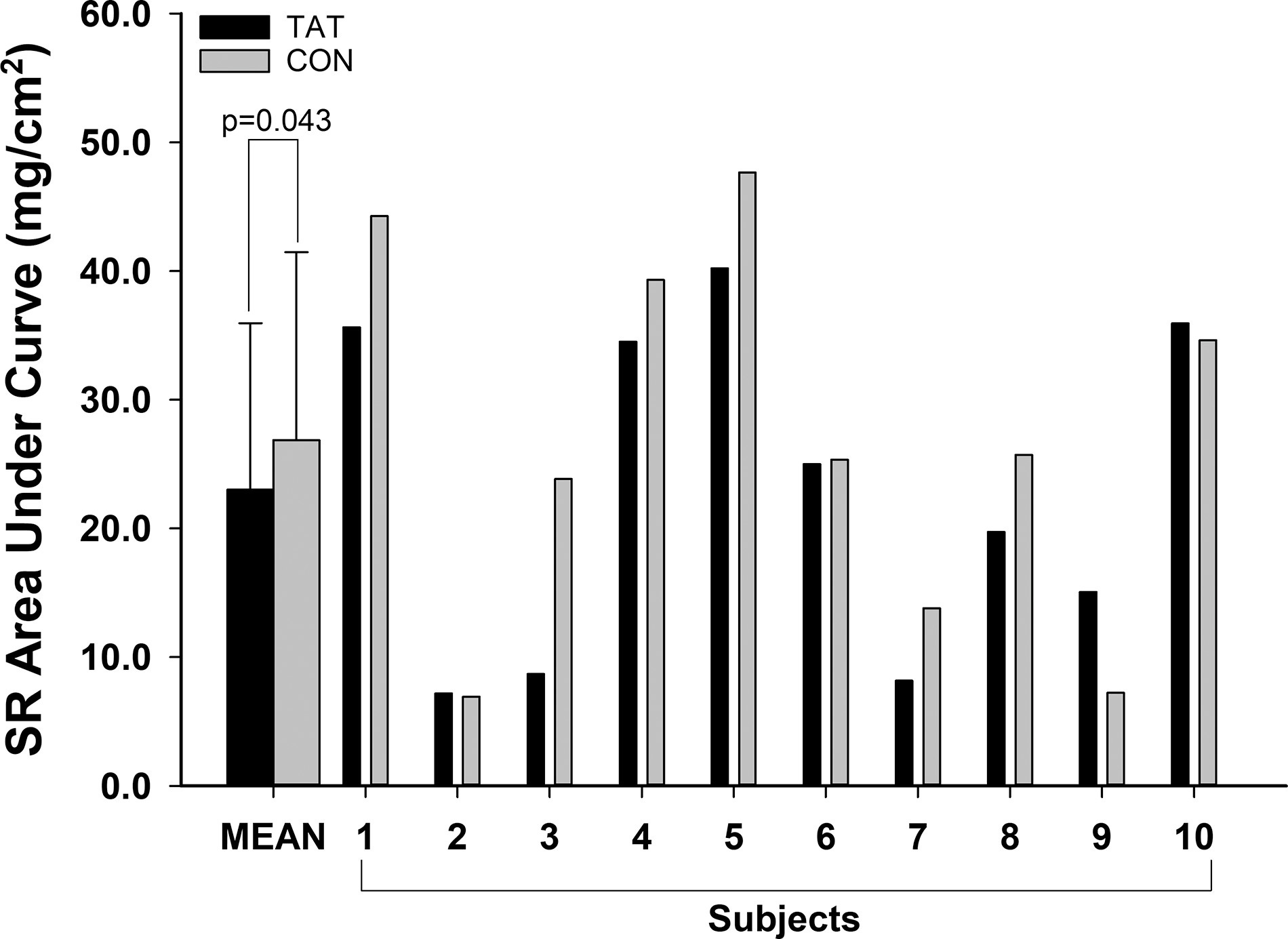
The research into sweating impairments (and for the record changes in sweat sodium) is not all in agreement though (which is often the case - remembering we are trying to be ‘less wrong’ in science). Some research has not shown changes in sweat rate. Of interest the research I found showing no change used exercise as the stimulus and this is not an irrelevant variable.
Take Home Message
Tattooed skin could well have an impairment in sweating, the theory being due to damage as a result of the tattooing process. This clearly would have a dose-response type of relationship, that is; the greater the surface area of tattoo as a percentage of body surface area the greater the impact. Similarly location probably matters to some extent though it is probably small. The implications of impaired sweating are real for those competing in hot environments and may become impactful with age too, as the elderly don’t thermoregulate quite as well.
Health
This article was largely inspired by recent media reports of increased malignant lymphoma rates in those who had tattoos. As an aside, this is quite interesting to me given the research that drove the media coverage was from mid 2024 (and there was another more recent study) which speaks to both the copycat nature of media and perhaps a slanted representation of news - this study is no more or less relevant now that it was when it came out, but let’s not get into it (I do also realise I am part of this to a degree, though I see this piece as more of an addition to provide context for readers who may have seen what I did).
The study in question was from Sweden and was a case control study. Epidemiology is almost nobody’s favourite topic but I have to do some explaining here for readers to understand context - I apologise in advance.
Study Design
Case-control studies are studies where scientists look at risk factors for a disease using a group with the disease and matching them with a ‘control’ group. In this situation; using malignant B cell lymphoma as the disease and evaluating tattoos as the exposure (in those with the disease and “controls” who don’t have the disease). These are retrospective studies (done after diagnosis), looking back at exposure.
The mirror of these is a cohort study, a forward looking study where we follow a ‘cohort’ of exposed individuals (prospectively) and track the incidence of an outcome. For the study in question, this would mean following a group of 5000 teenagers for 40 years and seeing their health outcomes, with the variable of interesting being whether they got tattoos or not (and using a large number to hopefully washout noise of other factors as much as possible) - you can see this isn’t really that feasible logistically.
So to review, we have 2 types of study, both with a 2x2 matrix (disease vs not and exposed vs not) but how we choose the groups varies. In one type (cohort) we chose a group and watched them get exposed or not, then develop the disease or not. In the other (case-control) we look at a group with the disease of interest, match them to people who are similar but without the disease and then look at the rates of the exposure of interest. Clear as mud, I know - don’t worry this stuff does students (me included) heads in all the time.
In the Swedish study mentioned, the population consisted of 11,905 individuals who were initially contacted. Remembering these were all people who had the outcome of interest (in this case malignant B cell lymphoma). The response rate was 54% among cases (n = 1398) and 47% among controls (n = 4193) - remembering that ‘cases’ had lymphoma and ‘controls’ did not, they were sourced from a national population registry rather than the national cancer registry. In this instance, researchers wanted 2 controls per case (don’t worry about why - it’s statistics). *Some responses (or non) were from families of deceased individuals given the nature of cancer.
What was Found?
The simple answer is increased risk. The statistically trained readers may be triggered by this, because classically the nature of a case-control study means that risk cannot be calculated. However, in certain cases this can be done, and this is one of those cases because ‘person time’ is available. In this case means this means we know when people got their tattoo and how long they were thus ‘exposed’. Again, it’s a weird technicality - don’t sweat it, I spent a long time wrapping my head around it (I am not a particularly statistically savvy guy).
Back to the study:
“We found that tattooed individuals had a 21% higher risk of overall malignant lymphoma compared with non-tattooed individuals, and that the association was strongest for diffuse large B-cell lymphoma and follicular lymphoma.”
We will talk about the implications of this soon - it’s probably not quite what you think. Having said that the authors gave some more colour that I found interesting too:
“The risk of lymphoma was highest in individuals with less than two years between their first tattoo and the index year (IRR = 1.81; 95% CI 1.03–3.20). The risk decreased with intermediate exposure duration (i.e., three to ten years), but seemed to increase again in individuals who received their first tattoo ≥11 years before the index year (IRR = 1.19; 95% CI 0.94–1.50). We found no evidence of an increased risk with a larger total area of tattooed body surface. On the contrary, we observed the highest lymphoma risk in individuals with tattoos smaller than one hand palm.”
The authors also found that tattoo removal increased risk of these cancers (numbers were small, unsurprisingly so this may be a statistical anomaly).
Will My Tattoo Give Me Cancer?
The most important first thing to discuss here is the statistics (I never thought I’d be this guy but here we are).
Risk and Base Rates
When authors mentioned an increased risk by 21% it is important to remember this is a RELATIVE risk. Meaning your risk goes from baseline to 21% more than that. Whilst everyone has their own risk profiles and thus base risk is hard to know on an individual level (and this 21% increase is a group average not the impact on the individual - for more about these concepts see this piece) we can get an indication of base rate in the population.
The base rate of malignant lymphoma varies, it’s higher in developed countries than developing ones (I have no idea why), globally it is 3.37%, though it has been increasing globally by ~3-4% per year though there has been some stabilisation in developed countries (Note; the article I got this info from is the best I can find but it is over a decade old). 2008 World Health Organisation data suggest the following rates of malignant lymphoma per 100,000:
Germany: 9.7
France (metropolitan): 12.07
United Kingdom: 12.92
United States of America: 16.11
So it’s likely that readers will have a risk that at baseline, at a population level, is between ~10-17/100,000, as such the tattooed amongst them have a rate of ~12.1-20.57/100,000. That is the ABSOLUTE risk increase (for a relative increase of 21%). Again, these numbers are all estimates and population level (got read the piece I linked to above about statistics, it covers the individual as part of a group) - but the point here is that even if this relative risk increase doubles the absolute risk to the individual doesn’t change a great deal for rare conditions.
What Can We Learn from Other Findings?
As highlighted above, there were some really interesting other findings from the study, including risk changes with duration. Risk was seen as high within the first 2 years of getting the tattoo and after 11. The former may be confounded by medical tattoos (often used in treatment planning for things like radiotherapy). There’s also a non-zero chance that certain individuals respond to tattoos in a way that means their progression to cancer is quicker (we aren’t getting into the pathophysiology of cancer but if you’re interested there’s reading out there - look into the “multi hit theory”). The longer duration uptick makes more sense when considering the contribution of chronic low grade immune response/inflammation in the development of cancer.
Similarly the finding of removal increasing risk, if not spurious given the small numbers, may reflect further damage beyond the initial insult of the tattoo - remember they are removed with lasers.
Is There Other Research?
There is a more recent study (from 2025), as mentioned earlier, which looked at similar cancers and skin cancer - which again makes some sense immunologically (we are injuring it and creating low grade inflammation in it). In short the study found:
A hazard ratio of 1.62 for skin cancer in those with tattoos- simplified this loosely means a 62% increase in risk of skin cancer. This was 1.33 (loosely 33% risk increase) in twins where one was tattooed and the other wasn’t.
This study found that there was greater risk with tattoos larger than palm sized. (Hazard Ratio of 2.37 or an increase in risk of roughly 137% for skin cancer of 2.97 or an increase in risk of roughly 197% for lymphoma)
*Hazard ratios refer more to risk at any moment in time whereas relative risks refer more to a cumulative risk.
What are the Implications of All of This?
Ultimately they are as they seem - a mildly increased risk of some cancers from baseline. Again, your individual risk will vary.
Whilst not getting a tattoo looks to reduce your risk of some cancers, the choice either way pales in comparison to the impact of things like smoking, exercise and sleep. It is worth noting, that behaviours compound also; for instance significant and regular sun burns, in addition to smoking, in addition to a tattoo likely compounds your risk of cancer at least to a degree (behaviours and their impacts do not exist in a vacuum).
I will close this piece out on a lighter note, with my favourite part of the 2024 Nielsen et al paper. It gives a good indication of how absurd science can be at times. Case-control studies are, because of their retrospective nature, prone to recall bias (mis-remembering). Addressing this is something authors should do, but it’s probably not quite as relevant to address in cases of things like whether someone had a child or not, graduated high school or university, you know - memorable life happenings. As such reading this made me giggle at the absurdity of what was almost certainly a reviewer request to address the risk of recall bias:
“We consider recall bias with respect to exposure status to be highly unlikely because getting a tattoo is an active decision underpinned by motivational factors such as achievement of milestones or expression of individuality or affection. In addition, we do not expect individuals with lymphoma to systematically misremember getting tattooed to a higher (or lower) extent than individuals without lymphoma, which would be the definition of recall bias within the current study design.”
Your choice of tattoos is your own, it’s probably less than perfect for health and aspects of performance, but so are many other behaviours we all engage in regularly. As always; focus on the big rocks for the largest impact in all realms of health and performance.
References
Baranska A, Shawket A, Jouve M, Baratin M, Malosse C, Voluzan O, Vu Manh TP, Fiore F, Bajénoff M, Benaroch P, Dalod M, Malissen M, Henri S, Malissen B. Unveiling skin macrophage dynamics explains both tattoo persistence and strenuous removal. J Exp Med. 2018 Apr 2;215(4):1115-1133. doi: 10.1084/jem.20171608. Epub 2018 Mar 6. PMID: 29511065; PMCID: PMC5881467.
Osilla EV, Marsidi JL, Shumway KR, et al. Physiology, Temperature Regulation. [Updated 2023 Jul 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507838/
Maurie J. Luetkemeier, Dustin R. Allen, Mu Huang, Faith K. Pizzey, Iqra M. Parupia, Thad E. Wilson, and Scott L. Davis. Skin tattooing impairs sweating during passive whole body heating. Journal of Applied Physiology. 2020, 129:5, 1033-1038
Luetkemeier MJ, Hanisko JM, Aho KM. Skin Tattoos Alter Sweat Rate and Na+ Concentration. Med Sci Sports Exerc. 2017 Jul;49(7):1432-1436. doi: 10.1249/MSS.0000000000001244. PMID: 28240705.
Rogers E, Irwin C, McCartney D, Cox GR, Desbrow B. Tattoos do not affect exercise-induced localised sweat rate or sodium concentration. J Sci Med Sport. 2019 Nov;22(11):1249-1253. doi: 10.1016/j.jsams.2019.06.004. Epub 2019 Jun 19. PMID: 31235387.
Nielsen C, Jerkeman M, Jöud AS. Tattoos as a risk factor for malignant lymphoma: a population-based case-control study. EClinicalMedicine. 2024 May 21;72:102649. doi: 10.1016/j.eclinm.2024.102649. PMID: 38827888; PMCID: PMC11141277.
Huh J. Epidemiologic overview of malignant lymphoma. Korean J Hematol. 2012 Jun;47(2):92-104. doi: 10.5045/kjh.2012.47.2.92. Epub 2012 Jun 26. PMID: 22783355; PMCID: PMC3389073.
Clemmensen, S.B., Mengel-From, J., Kaprio, J. et al. Tattoo ink exposure is associated with lymphoma and skin cancers – a Danish study of twins. BMC Public Health 25, 170 (2025). https://doi.org/10.1186/s12889-025-21413-3
Years back at the American College of Sports Medicine conference (ACSM), I saw a research poster about how tattoos affect sweating. It really made me stop and think - what a cool idea to study. And it made sense - dye was being injected below the skin at a level that could potentially block the sweat glands.
There are a few studies at this (one example below), and I haven't gone through these thoroughly, but it's an interesting topic. From my understanding, studying sweating is REALLY nuanced, because the techniques that can be used to quantify it precisely can also influence sweating rate.
Example study: https://journals.physiology.org/doi/full/10.1152/japplphysiol.00427.2019
This is not at the "do tattoos cause lymphoma" level but some potentially really interesting science!
So good.