

You Should Probably Be Taking Creatine
You Should Probably Be Taking Creatine
The why, how and when


Image by freepik
Whilst this probably dates me, I remember being in high school where there was significant controversy that one of my fellow students was using creatine to aid him in the gym. It was spoken about as though it was very murky ethically and dangerous to boot. With the time that has passed the supplement has gone from fringe, questionably used supplement to one of the most researched, safe and evidence backed supplements available.
Evidence was initially predominantly strength related, but as time passes benefits continue to become more wide ranging. Understanding the biochemistry of creatine, it is logical that it has since been found to aid most anaerobic activities.
Of more surprise and perhaps interest, is the more recent (and currently less abundant) research on its nootropic effects. These are more pronounced in those with a low creatine diet (which makes complete sense) but seem to extend to others too. It may be a little too early to recommend creatine for nootropic effects, and possible mental health effects but this depends on your personal lenses that you use for decision making (see my article on my lenses here which explains why I think most should be using creatine).
There is also some suggestion of creatine having anti-inflammatory and antioxidant effects. Likewise, there is some literature pertaining to creatine’s use in mild traumatic brain injury, with somewhat more evidence in favour of prevention rather than treatment. It is however, too early to be sure of the positive effects, although as acknowledged above, personal lenses may tip the balance of this decision making.
What is creatine?
Creatine is an amino acid, naturally occurring in the body. It is made in the liver, pancreas and kidneys but can be made synthetically also (this is the way the supplements are made).
It is available in meat and fish, which explains the benefits shown in supplementation for those who do not eat meat.
It is stored mostly in muscles and used by the body primarily at times of high energy requirements as a phosphate donor to aid in energy production.
Who Needs Creatine?
Everyone, but not everyone needs to supplement. It seems increasingly likely that a trial of supplementation is reasonable even for high meat consumers given the cost of creatine, its risk-benefit profile and high potential for positive outcomes.
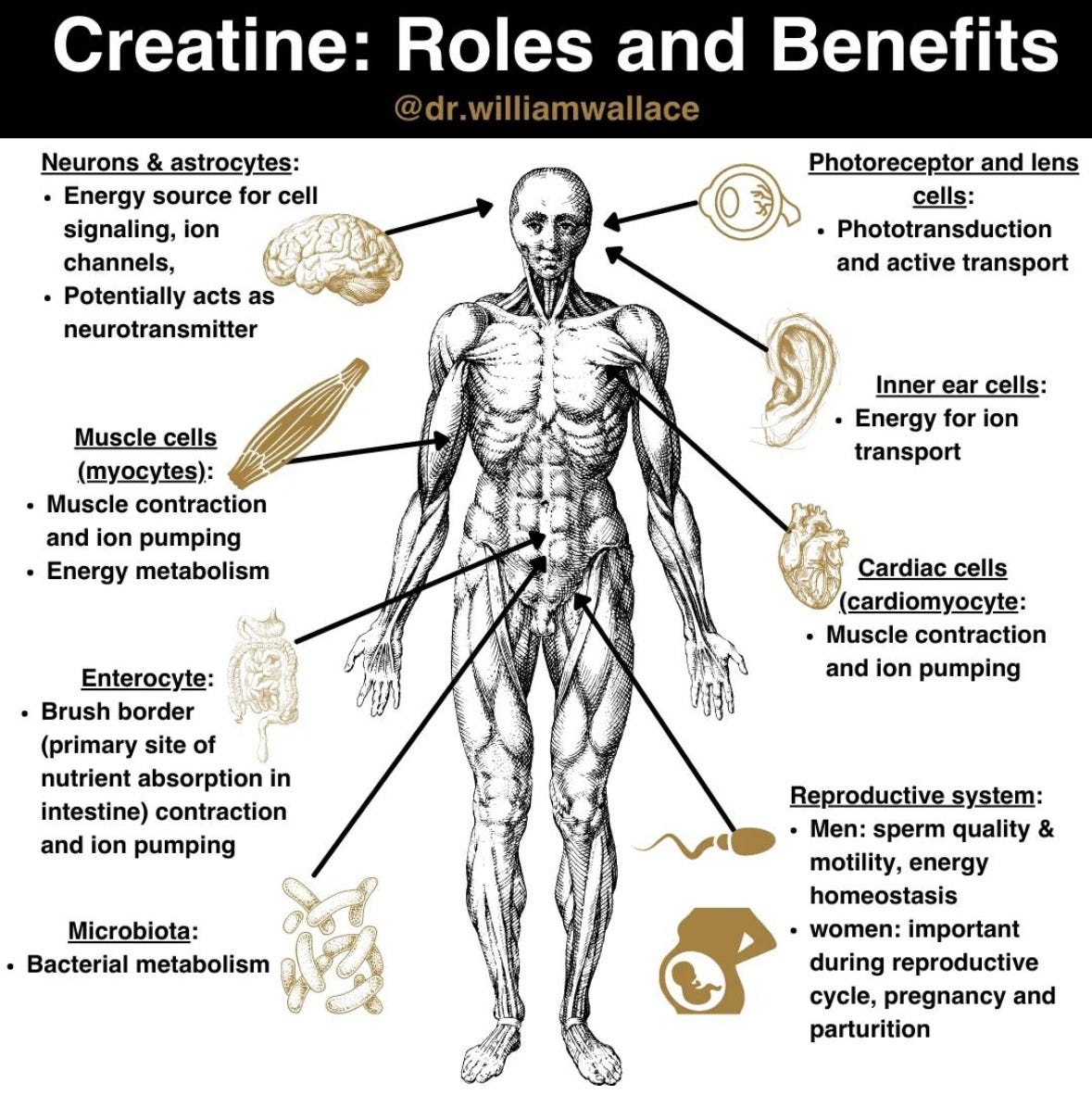
Image courtesy of William Wallace
How Much Should I Take?
Most research uses classical dosing protocols involving a loading phase and then a maintenance phase. In typical fashion, once this was used in the scientific literature it becomes the standard protocol, and thus is repeatedly used.
So most research uses these sort of dosing protocols (0.3g/kg/day for 3 days, maintenance dosage of 0.03g/kg/day for a 75kg person this translates to 22.5g/day for 3 days, and 2.25g/day thereafter) and often would cycle people off of it after 3 weeks. This is sometimes simplified to a 20g/day loading dose and 3-5g/day maintenance dose.
That said, enough evidence exists, in addition to common sense in that many people get good amounts of creatine from their diet, that it can be supplemented without cycling off of it and at a daily dose without need for loading doses. Most people take 3-5g/day (looking at the maintenance dose this makes sense for the much of the adult population) but some people who are much heavier use higher doses. The risk here being some gastrointestinal upset, though dosing can be split across the day rather than taken in a single dose which helps the tolerability of creatine.
When Should you Take Creatine?
The answer is whenever you’ll remember to take it. In reality it’s not a huge deal, it’s predominantly a chronic dosing effect so dose timing is less important. That said, there’s some research that it helps glycogen resynthesis post exercise, so if that’s a priority then maybe take it there.
What Type and Where from?
As mentioned, it is present in meat and fish, but even in those who consume a lot of these it likely has benefits.
It is sold in many forms, but monohydrate is the cheapest, most widely researched and I am yet to see evidence that other types are better for anything aside from reducing the weight of your wallet, though as always, I am happy to be proven wrong.
One crucial aspect here is around supplement quality. This point cannot be overstated, the industry is one which can be a bit of a wild west in some regards. Make sure you are buying supplements from reputable sources, I would always recommend brands that undergo third party batch testing to help reduce the risk of contamination and ensure purity. If you are an athlete who gets drug tested then you’d need something that is informed sport certified or similar, but you’d know this already.
Side Effects
Gastrointestinal distress in the form of diarrhoea, vomiting and stomach cramps are the most common issues but are rarely present if not ingesting amounts used with loading protocols (>10mg in a single dose). These are mostly avoided through adequate water consumption and splitting high doses across the day.
The other reported side effect which bothers some more than other is water retention. Creatine will draw water with it, thus increasing total body water and as a result both water retention and scale weight. The take home message here being, if you want to look leaner, maybe cycle off of it and likewise if the scale number goes up and you look a little puffier, don’t be surprised. I am increasingly less convinced this effect is of significance for most people and these authors agree.
There is also an associated increase in creatinine which is related to metabolism of creatine and not kidney damage (as can be a concern when this rise is otherwise unexplained) so it serves you to alert your doctor to you taking creatine (or indeed cycling off of it if you are getting blood tests for fear of being told your kidney function is not optimal).
Special Interest Groups
The evidence for benefits of creatine looks to be more pronounced in low meat consuming populations and the elderly.
Athletes are the most well-researched group for creatine use with the highest level of evidence existing for its benefits and subsequent recommendation by most sport nutrition bodies for performance.
As mentioned there is active research and ever evolving science in the brain and mental health spaces too. There’s also some research published in September showing benefits of creatine in long covid.
Things to Note
It is acknowledged that there are responders and non-responders to creatine supplementation, and as the name suggests the latter of the two groups may well not see a great benefit of supplementation. The differences between the two have been investigated somewhat and the key differences seem to be somewhat unsurprising. The pre-supplementation levels of creatine are lower in responders (so by supplementing the deficit is corrected) and responders also have a higher proportion of type II muscle fibres (commonly known as fast twitch muscle fibres). The latter of these makes some sense when looking at the physiological differences between type II and type I muscle fibres, the former being a more fast twitch type of person and thus more anaerobic/glycolytic and thus probably utilising more creatine.
My Take
I don’t see much downside, even in non-responders. Creatine is cheap, has minimal downside or side effects and has a potential upside.
I am fairly bullish on the potential for creatine therapeutically in traumatic brain injuries and smart people are already recommending it post concussion (I will write an article on this soon so subscribe above to make sure you don’t miss it).
Make sure you are getting your diet right as the predominant factor before supplementation as mentioned in this article previously.
For more on creatine check out Examine’s summary
Reference List
Konstantinos I. Avgerinos, Nikolaos Spyrou, Konstantinos I. Bougioukas, Dimitrios Kapogiannis.Effects of creatine supplementation on cognitive function of healthy individuals: A systematic review of randomized controlled trials.Experimental Gerontology, Volume 108. 2018, Pages 166-173. https://doi.org/10.1016/j.exger.2018.04.013
Ainsley Dean, P. J., Arikan, G., Opitz, B., & Sterr, A. (2017). Potential for use of creatine supplementation following mild traumatic brain injury. Concussion, 2(2), CNC34. doi:10.2217/cnc-2016-0016
Dolan, E., Gualano, B., & Rawson, E. S. (2019). Beyond muscle: the effects of creatine supplementation on brain creatine, cognitive processing, and traumatic brain injury. Eur J Sport Sci, 19(1), 1-14. doi:10.1080/17461391.2018.1500644
Kreider, R. B., Kalman, D. S., Antonio, J., Ziegenfuss, T. N., Wildman, R., Collins, R., . . . Lopez, H. L. (2017). International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. J Int Soc Sports Nutr, 14, 18. doi:10.1186/s12970-017-0173-z
Lugaresi, R., Leme, M., de Salles Painelli, V., Murai, I. H., Roschel, H., Sapienza, M. T., . . . Gualano, B. (2013). Does long-term creatine supplementation impair kidney function in resistance-trained individuals consuming a high-protein diet? J Int Soc Sports Nutr, 10(1), 26. doi:10.1186/1550-2783-10-26
Nelson, A.G.; Arnall, D.A.; Kokkonen, J.; Day, R.; Evans, J. Muscle glycogen supercompensation is enhanced by prior creatine supplementation. Med. Sci. Sports Exerc. 2001, 33, 1096–1100.
Elstad, K.; Malone, C.; Luedke, J.; Jaime, S.J.; Dobbs, W.C.; Almonroeder, T.; Kerksick, C.M.; Markert, A.; Jagim, A.R. The Effects of Protein and Carbohydrate Supplementation, with and without Creatine, on Occupational Performance in Firefighters. Nutrients 2023, 15, 5134. https://doi.org/10.3390/nu15245134
Roschel H, Gualano B, Ostojic SM, Rawson ES. Creatine Supplementation and Brain Health. Nutrients. 2021 Feb 10;13(2):586. doi: 10.3390/nu13020586. PMID: 33578876; PMCID: PMC7916590.
Candow, D.G., Forbes, S.C., Ostojic, S.M. et al. “Heads Up” for Creatine Supplementation and its Potential Applications for Brain Health and Function. Sports Med 53 (Suppl 1), 49–65 (2023). https://doi.org/10.1007/s40279-023-01870-9
Jose Antonio, Darren G. Candow, Scott C. Forbes, Bruno Gualano, Andrew R. Jagim, Richard B. Kreider, Eric S. Rawson, Abbie E. Smith-Ryan, Trisha A. VanDusseldorp, Darryn S. Willoughby & Tim N. Ziegenfuss (2021) Common questions and misconceptions about creatine supplementation: what does the scientific evidence really show?, Journal of the International Society of Sports Nutrition, 18:1, DOI: 10.1186/s12970-021-00412-w
Slankamenac, J., Ranisavljev, M., Todorovic, N., Ostojic, J., Stajer, V., & Ostojic, S. M. (2023). Effects of six-month creatine supplementation on patient- and clinician-reported outcomes, and tissue creatine levels in patients with post-COVID-19 fatigue syndrome. Food Science & Nutrition, 11, 6899–6906. https://doi.org/10.1002/fsn3.3597
Great reading David, a topic that has been a subject of much debate in rugby circles for years. Creatine's evolution from a supplement shrouded in controversy to one recognized for its myriad health benefits underscores the dynamic nature of sports nutrition and supplement research.
Given the physical demands of rugby, where high-intensity training is routine, and the risk of injury is ever-present, creatine's role in muscle recovery and injury prevention becomes particularly relevant. Thus, what role does creatine play in muscle recovery and injury prevention in high-intensity training, especially in a sport as physically demanding as rugby?
Well balanced and informative writing on the topic thanks David. I have been taking 5 grams daily of creatine monohydrate since the late nineties. I have read contradictory reports on the effect of creatine on plasma homocysteine levels, i.e., some studies showing an increase and others a decrease in homocysteine levels. I am particularly interested about any possible impacts on cardiovascular health via this pathway. I was wondering if you have any opinion or knowledge of creatine and homocysteine levels?